




Introduction
“Change is the only constant”. This past year has continued to show how profoundly true this adage is, in both the global health sector and the world at large. Together, we face the interconnected but independent triple threat of COVID-19, the Climate Crisis and growing global instability leading to devastating new and protracted Conflicts. Underpinning these three ‘C’s is a deepening of the inequities that jeopardize the health and rights of women, youth, children, and their communities. This year certainly does not mark the first time the world has faced these issues. Yet the pace of change has made it difficult to find our footing – let alone make meaningful progress.
Constant change can seem overwhelming, but it can also bring with it opportunities for reflection and creativity. This past year has also brought remarkable and much needed change to our sector in terms of the power of information.
Community-led, anti-colonial, and localized orientations to global cooperation and evaluation are no longer framed as ‘interesting discussions’ but urgent priorities demanding our attention. We are adapting to virtual methodologies and challenging long-held assumptions about how evaluation is done and for whose benefit it is undertaken. For the first time, we have sector data on anti-racism efforts in our organizations and operations, and we are talking about the foundational change that is needed to actively resist racism in our work. We are also sharing information on an unprecedented scale, with more and more organizations and funders committing to transparent and timely data communication, both domestically and globally.
Within CanWaCH, 2021 was also a year of renewal and growth. We have moved into a new chapter of our mandate, guided by a strategic plan that will guide us for the next 5 years. As part of this, CanWaCH has made an explicit commitment to advancing thought leadership, mobilizing evidence, and deepening partnerships. This annual Global Health Impact Report is one channel through which we action this commitment, and in the years to come, we anticipate co-creating a variety of guides, tools and research to inform, inspire and empower our sector. Co-creation is the key – together with you, we aim to identify and prioritize those topics that will make the greatest impact for the lives and rights of people worldwide.
This year’s report is more compact than some of our previous reports, reflecting the fact that much of this year was spent re-evaluating and reorganizing our approaches amid a changing world. We hope that the data within it is as useful as always, and that the future reflections on evidence gaps and opportunities will provide a launch point for the deep work we will embark on together in the year ahead.

In solidarity,
Julia Anderson, CEO
Methodology
The CanWaCH Project Explorer provides valuable aggregate analysis of the scale and scope of Canada’s work in global health and gender equality since 2010, along with interactive digital tools for analysis and interpretation. It captures projects from CanWaCH members and non-members, including Canadian and non-Canadian civil society organizations, academia, multilateral institutions, bilateral commitments, and private sector actors.
The data included in this report is a culmination of multiple targeted outreach efforts by CanWaCH to members and non-members, supplemented by or triangulated with online search of websites and published materials, including the Global Affairs Canada Project Browser. Organizations are also able to contribute data at any time of year, via CanWaCH’s Project Explorer platform. In all cases, CanWaCH collects robust data across 20 primary data fields. Data is sourced in either English or French, and translation to the other official language is provided by CanWaCH. Unless otherwise specified, all financial figures presented in this report are in Canadian dollars.
As the Project Explorer is a living tool generated with the sector from projects that are very new or have long-since closed, it contains some projects that have limited available data. It may also not include data on active projects that, for reasons of safety for participants and staff, cannot be fully disclosed publicly. Wherever relevant, sample sizes are noted. While numbers are accurate at the time of publication, please visit the website for the most recent figures. As always, we are particularly grateful to the CanWaCH Metrics Working Group for their contributions to our work and analysis. Our methodology and standard operating procedures are available here.
Project Explorer Data
Data for this report was extracted from the CanWaCH Project Explorer, an open access tool that showcases the full spectrum of Canadian contributions in global health and gender equality through interactive maps, visuals and detailed project-level data. This includes a wide range of data on projects funded by the Government of Canada as well as other funding sources. The Project Explorer currently holds 13181 development and humanitarian initiatives from 2010 to present, spanning across 158 countries, with a total combined funding of CAD $15,509,912,828.
1 Sample size: 1318 from all available funding sources
A Global Snapshot
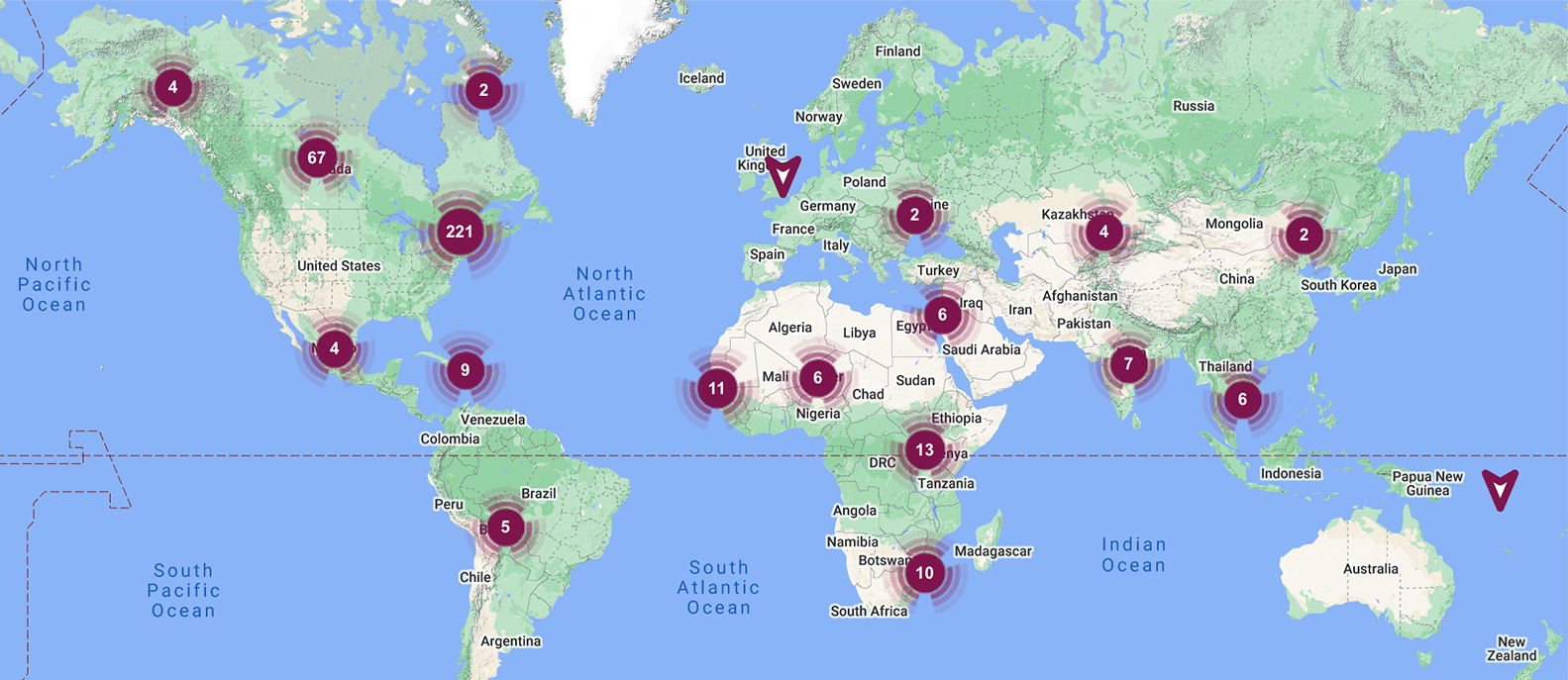
Where We Work
During the period analyzed (2020-2021), the following countries received the highest overall amount of funding from the reported projects:
Top 10 countries by Total Value of Reported Projects2
| Rank | Country | Total Combined Value of Reported Projects |
|---|---|---|
| 1 | Tanzania | $752,563,424 |
| 2 | Ethiopia | $736,918,111 |
| 3 | Bangladesh | $647,870,204 |
| 4 | Afghanistan | $644,735,344 |
| 5 | Mali | $606,845,367 |
| 6 | Haiti | $583,099,701 |
| 7 | Mozambique | $574,150,143 |
| 8 | Ghana | $481,168,888 |
| 9 | South Sudan | $470,042,922 |
| 10 | Nigeria | $344,443,540 |
2 Sample size: 1039 projects
What We Work On
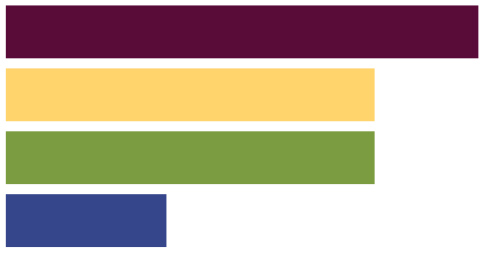
In terms of priorities, the global health issues with the most fund allocations between 2010 and 2021 were:
Top 5 Global Health Areas of Focus3 by Total Value of Reported Projects
| Rank | Area of Focus | Total Combined Value of Reported Projects | Percentage Distribution Amount |
|---|---|---|---|
| 1 | Infectious & Communicable Diseases | $2,543,644,158 | 27.85% |
| 2 | Nutrition | $1,607,307,764 | 17.60% |
| 3 | Sexual Health & Rights4 | $1,324,032,306 | 14.50% |
| 4 | Reproductive Health & Rights incl. Maternal Health4 | $1,098,132,945 | 12.02% |
| 5 | Primary Health Care | $1,026,177,454 | 11.24% |
3 Sample size: 833 Projects
4 Sexual health and rights includes activities regarding sexually transmitted infections, sexual relationships, discrimination based on sexuality, etc. Reproductive health and rights, including maternal health, includes all aspects of reproductive functioning including maternal care, family planning, safe abortion access, etc.
Who We Work With
From a subset of projects reporting population data3, projects are reaching or planning to reach at least:
people of all ages and genders
93 countries
$5,022,121,580
3 Direct population sample size: 520 projects with a total reach of 1.802,507,875 people. Indirect population sample size: 146 projects with a total reach of 196,894,132 people. Please note: projects include information on population reached (achieved or expected), including the direct population served as well as the indirect population reached if applicable. The figures given here reflect the sum of all numbers available in the Project Explorer, irrespective of project budget, area of focus, and population details.
4Population numbers reflect figures as reported from contributing organizations. Contributors are given guidelines to ensure reporting consistency and to avoid double-counting.
From those projects that shared data on target population by age and gender5,

| 59% of projects included adult women (18+ years) | 63.5% of projects included adolescent girls |
| 88.2% of projects included girls over 5 years | 21.1% of projects included senior adult women |
5 Sample Size with target population age and gender reported: 502 projects
| 59% of projects included adult men (18+ years) | 46.2% of projects included adolescent boys |
| 46.2% of projects included boys over 5 years | 20.5% of projects included senior adult men |
From those projects that shared data on target population by other population descriptors6
| 68.2% of projects were implemented in Rural settings | 25.7% of projects were implemented in Urban settings |
| 20.4% of projects served internally displaced people | 14.3% of projects served persons with disabilities |
| 13.1% of projects served refugee communities | 3.7% of projects served local minority groups |
| 2.4% of projects served Indigenuous peoples | 2.0% of projects served LGBTQ2I communities |
6 Sample Size with target population descriptors: 245 projects
Data Spotlight: Sexual and Reproductive Health & Rights
In 2017, the Government of Canada made a significant investment in sexual and reproductive health and rights (SRHR) by committing $650M over three years (2017-2020). The CanWaCH Project Explorer database contains a comprehensive list of the projects funded under the investment.
At a glance: SRHR
Projects were implemented across 56 countries, and led by 68 unique partners:
| 74% NGOs |
| 15% Multilaterals |
| 11% Others |

| 57% was allocated to multilaterals |
| 25% was allocated to Non-Canadian Partners (NGOs, academic institutions and other public sector) |
| 18% was allocated to Canadian partners (NGOs, government, and private sector) |
Investment in the Neglected Areas of SRHR
Based on a review of project information, we have concluded that data remains limited in terms of the scale and impact of projects which specifically address frequently neglected areas of SRHR; namely:
- Adolescent SRHR (including comprehensive sexuality education)
- Comprehensive Contraceptive Care
- Safe and Legal Abortion
- Support for Advocacy relating to SRHR
As a result of dedicated data collection efforts earlier this year, CanWaCH collected programmatic data on the neglected areas of SRHR directly from Canadian-based and global civil society organizations funded under the Global Affairs Canada investment in order to estimate the extent to which the neglected areas are currently addressed. Between July-August 2020, CanWaCH implemented a ‘data drive’ to gather detailed data on programming in the neglected areas of SRHR. A custom data collection form, using CanWaCH’s Project Explorer standard data fields as a basis, was developed and sent to 33 Canadian-based and global civil society organizations funded under the $650M SRHR funding envelope. These organizations were identified using the available published list of projects provided by Global Affairs Canada, as well as CanWaCH’s existing database.
Overview of CanWaCH Analysis
31
$262,504,105
| Neglected Area category | Number of projects | % of projects |
|---|---|---|
| Adolescent SRHR (including comprehensive sexuality education) | 19 | 61.3% |
| Comprehensive Contraceptive Care | 21 | 67.7% |
| Safe and Legal Abortion | 9 | 29% |
| Support for Advocacy | 17 | 54.8% |
| Total Projects | 31 | – |
Population Reach: Respondents reported reaching a total of 19,049,882 people (directly and indirectly) across 30 projects with Adolescent SRHR having the highest reach and Support for Advocacy having the lowest reach.
Population Groups: Adults and adolescents were cited as the main population groups targeted by these projects. Overall, more adult females and adolescent girls were reported as target demographics; however, men and adolescent boys were cited across all neglected areas as also being targeted through activities. Adolescent girls were not reported to be one of the main target groups for Comprehensive Contraceptive Care or Safe and Legal Abortion.
Outputs: The top three outputs the most commonly cited with the most reach were (in order):
- People trained: examples include health service providers, teachers, peer educators, personnel/staff, government officials, and community members
- Awareness campaigns: examples include outreach activities and learning events conducted, and people reached through these events.
- SRHR services provided: examples include adolescent girls and young women linked to referral services, including family planning, contraceptives, post-abortion care, and sexual and gender-based violence
- Indicators: The most common of the standard SRHR KPI indicators measured were related to Adolescent SRHR while the least common were related to Safe and Legal Abortion.
CanWaCH is very pleased by the decision this year by Global Affairs Canada to establish three Canada-specific data tracking codes relating to SRHR:
- 13011: SRHR Advocacy and Reform
- 13012: Comprehensive Sexuality Education
- 13021: Safe Abortion Services and Post-abortion care
The addition of these codes, combined with the uses of the ‘adolescent policy marker’ will significantly improve future analyses in SRHR data, and we look forward to revising the above analysis in future based on these codes.
Emerging Data: Humanitarian Initiatives
CanWaCH’s Project Explorer has begun to capture more humanitarian initiatives as part of our commitment to better understanding investments in this area. To date, the Project Explorer features a sample of over 144 projects with a focus on Humanitarian Response (2010-present). Total combined funding amount for all projects with a focus on humanitarian response $732,476,548. Data in this area must be interpreted carefully, and it should not be considered representative of the entirety of Canadian investments in humanitarian action.
Where We Work: Humanitarian
50 Countries with projects with a focus on Humanitarian Response:
Top 5 countries by Total Value of Reported Projects
| Rank | Country | Total Combined Value of Reported Projects |
|---|---|---|
| 1 | Syrian Arab Republic | $46,349,191 |
| 2 | Iraq | $44,007,189 |
| 3 | South Sudan | $35,530,000 |
| 4 | Lebanon | $31,925,300 |
| 5 | Bangladesh | $23,722,212 |
Who We Work With: Humanitarian
From a subset of projects reporting population data7, the initiatives reported reaching at least:
people of all ages and genders
29 countries
$268,286,857
7 Sample size of projects: 66 projects
Total population reach:
10,761,627
581,883
Reporting Organizations: Humanitarian
43 Reporting Organizations have shared that they have worked or are currently working on Canadian humanitarian projects.
| Total number of unique reporting organizations | Canadian-based | Other countries | Total |
|---|---|---|---|
| NGOs | 18 | 11 | 29 |
| Academia & Research | 1 | – | 1 |
| Private Sector | 1 | 1 | 2 |
| Multilateral | – | 9 | 9 |
| Government & Public Sector | 2 | – | 2 |
| Total | 22 | 21 | 43 |
Emerging Data: Domestic Efforts
The Project Explorer captures global health and gender equality efforts around the world, but also within Canada. An increasing number of Canadian actors in the global health and rights sectors are scaling up domestic engagement, and accordingly, we have seen more reports of Canadian-based work in our Project Explorer than ever before. For the first time, our sector will be able to capture and share the full spectrum of organizational efforts in Canada to advance gender equality and social justice.
For our part, the Equal Futures Network is a CanWaCH initiative that seeks to connect national, regional, community and grassroots organizations, agencies and projects from across Canada that are committed to advancing gender equality. It provides a platform for diverse partnerships and collaboration in order to drive progress in achieving gender equality and empowerment.
As of this report, there are 407 Canadian organizations in our database with development initiatives across Canada, including 390 who are part of the Equal Futures Network.
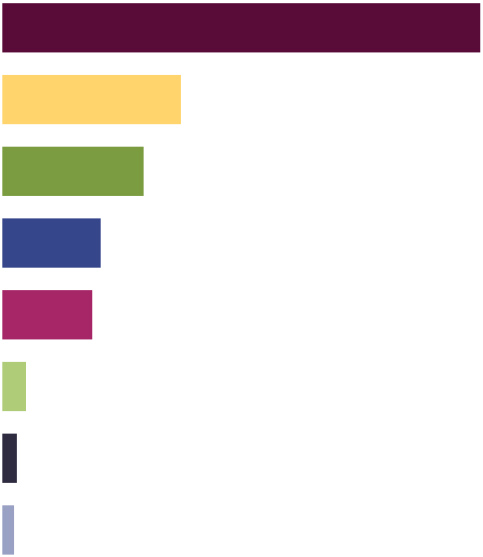
What We Work On: Domestic Efforts
Top 10 Reported Areas of Work (2021)8
| Rank | Scope of Work | Percentage |
|---|---|---|
| 1 | Education/Workshops | 58% |
| 2 | Advocacy/Campaigns | 48% |
| 3 | Front line service delivery/Support Services | 39% |
| 4 | Gender Based Violence | 29% |
| 5 | Empowerment | 23% |
| 6 | Sexual and reproductive health and rights (SRHR) | 14% |
| 7 | Network | 13% |
| 8 | Research/Academia | 11% |
| 9 | Entrepreneurship/Social Enterprise/B-corp | 9% |
| 10 | Employment/Professional Training | 8% |
8 Sample size of organizations: 390 organizations
Who We Work With: Canadian Efforts
Top 9 Engaged Communities9
| Rank | Communities | Percentage |
|---|---|---|
| 1 | BIPOC communities | 54% |
| 2 | Youth | 51% |
| 3 | 2SLGBTQ+ communities | 49% |
| 4 | Immigrants, new Canadians or refugees | 40% |
| 5 | Individuals with disabilities | 30% |
| 6 | Francophone communities | 28% |
| 7 | Rural and/or Northern communities | 26% |
| 8 | Other | 18% |
| 9 | Seniors | 16% |
9 Sample size of organizations: 390 organizations
Reporting Organizations: Canadian Engagement
Top 9 Reported Organization Structures10
| Rank | Communities | Percentage |
|---|---|---|
| 1 | Women-led | 76% |
| 2 | Small/grassroots organization | 33% |
| 3 | Youth-led | 16% |
| 4 | Volunteer-led | 16% |
| 5 | 2SLGBTQ+ -led | 14% |
| 6 | Black or POC-led | 7% |
| 7 | Indigenous-led | 7% |
| 8 | Immigrant, new Canadian or refugee-led | 4% |
| 9 | Other | 4% |
10 Sample size of organizations: 244 organizations
Innovation in Data
Between 2018-2021, the Canadian Collaborative for Global Health brought together Canadian and global partners to generate innovative solutions to urgent data challenges in global health and gender equality where Canada has made significant contributions to date, and where significant gaps in data capacity, knowledge, or resources remain. This effort was rooted in a feminist approach to creating lasting change, and was intended to enable Canada to meaningfully progress towards the SDGs. The following section summarizes the key deliverables and findings from the first round of this exciting initiative (September 2018 – June 2021).
Given the inspiring outcomes and positive feedback received from stakeholders and partners, CanWaCH was delighted to launch the second iteration of the Canadian Collaborative for Global Health in November 2021. While adjustments have been made to the structure of the initiative in response to feedback from stakeholders and the reality of a COVID-19 context, the core focus on data innovation remains consistent. We look forward to announcing the selected projects from our new cohort in Spring 2022.
Context
Between 2016 and 2018, CanWaCH listened to and consulted with our sector through a variety of methods to pinpoint obstacles to our collective success in achieving the targets laid out in the SDGs. What we heard:
- Data and data collection gaps – areas where data is lacking or remains difficult to collect and analyze – persist, particularly with regard to fragile contexts, marginalized communities, and outcome-level measurement.
- Where data and data collection resources exist, they may be inaccessible or go unused for a variety of reasons, leading to duplication, lack of uptake by communities, inefficient programming, and other issues.
- Perceived capacity to implement existing solutions or adopt explicitly feminist approaches remains limited for many Canadian actors, particularly in the above contexts. Specifically, lack of resources, skills, and meaningful linkages with other stakeholders repeatedly emerged as obstacles.
In response, CanWaCH launched the inaugural Canadian Collaborative for Global Health (the ‘Collaborative’) in 2018 with support from Global Affairs Canada. Through a competitive call for proposals, CanWaCH received 44 applications (38 in English, 6 in French) for this inaugural competition, representing 160 unique Canadian and global partners.
The Collaborative had three core objectives:
- Investigate the underlying barriers to effective data progress in areas of global health and gender equality: undertake rigorous research on the data challenge which the Lab seeks to address, including documenting existing approaches, to fully situate, support, and assess the proposed solution.
- Incubate useful solutions and effective partnerships to address these challenges: produce and pilot solutions to address the identified data gaps, leveraging interdisciplinary partnerships.
- Inspire and train the next generation of Canadian leadership in global health and gender equality metrics: develop the means by which data professionals and practitioners can learn about and be trained in the use of the solution(s) and its implications for their work.
As a result of the Collaborative, three key outcomes were expected from each Lab:
- Improved understanding of barriers affecting data collection, analysis, utilization, and communication.
- Increased availability of solution(s) and quality partnerships to inform programing, planning, and learning.
- Enhanced capacity of future researchers, civil society professions, and in-country leaders to collect, analyze, communicate, and use data effectively.
2018-2021: By the Numbers
Ultimately, six projects were selected for the inaugural initiative. Projects were co-led by 17 Canadian organizations and institutions, along with dozens of global partners including NGOs, global academia, and multilateral organizations.
Canadian Partners
| Canadian academic and research institutions: 59% |
| Canadian civil society organizations: 41% |
Other Partners
| Academic and Research Institutions: 63% |
| Non-Canadian NGOs (including International and National NGOs): 26% |
| Multilateral organizations: 11% |
The top six countries by budget allocation included Ethiopia, Vietnam, Senegal, Tanzania, Somalia, and Afghanistan.
100% of projects reached both adult women and men (18+ years) through their work. In addition, projects reached:
| 83% Adolescent girls | 33% Adolescent boys |
| 17% Girls and Boys over 5 years | 17% Children under 5 years |
| 33% Refugee and internally displaced populations (all ages and sex) |
Lab 1: Adolescent sexual and reproductive health and rights: Generating evidence and strengthening country capacity

Challenge
Sexual and reproductive health and rights (SRHR) are a priority area in global health and development efforts. Understanding how gender and other inequities impact SRHR, and specifically adolescent sexual and reproductive health (ASRHR), is crucial to developing programs and meeting the global goals. Challenges to the generation and use of ASRHR data include the sensitive nature of the topic, leading to questions about the data’s accuracy as well as how data is analyzed and communicated. National policy makers, researchers, NGOs and SRHR practitioners, among others, need data in order to build evidence on interventions and better understand ASRHR.
Key Issues:
- Missing Data: Data on the youngest adolescent age-cohorts are lacking. The reporting of sensitive events that are critical to measuring ASRHR and gender-related indicators (e.g. sexual behaviour, substance abuse, abortion and violence against women) are not captured because of low reporting.
- Weak Evidence to Action: Knowledge generation and use of evidence on ASRHR and related gender issues are weak and are not being harnessed effectively.
- Analytical Capacity: Institutional capacity in-country is often inadequate for effective analysis and communication of ASRHR data. Available ASRHR and related gender data through surveys are poorly harnessed by policy makers, program staff and project managers.
- Reliability in Data: Available ASRHR data are ignored due to low confidence in research quality across data collection methods – varied among self-reports in surveys, health facility data or qualitative studies.
Select Results
This project addressed some of the challenges inherent in the measurement and monitoring of ASRHR and related gender indicators in sub-Saharan Africa by developing novel mixed-methods research approaches for better measurement of ASRHR and coverage and gaps in services for adolescents. While partners collaborated with researchers from 10 countries in Sub-Saharan Africa, the in-depth work took place in Tanzania.
Use of existing data sources
Existing national surveys, such as the Demographic and Health Surveys (DHS) or other population level-data, can provide data that are of higher quality and widely available for a number of ASRHR indicators. Given that multiple time points are available (typically in four-year intervals) the data can also be used to assess trends in these indicators over time. A technical workshop was organized in Addis Ababa, Ethiopia in June 2019 to explore the potential for further ASRHR analyses of existing datasets. It was concluded that it is possible to obtain detailed and robust information on inequalities with national surveys even though sampling errors are larger with increased disaggregation, for instance, triple disaggregation with regards to inequities or moving beyond provincial or regional estimates to district level.
Collecting quantitative survey data with ACASI
Two surveys were conducted: an ASRHR survey using an Audio Computer-Assisted Self-Interview (ACASI) method, and a face-to-face survey with all women of reproductive age (WRA) living in Kisesa that included questions pertaining to women’s experience with the COVID-19 pandemic. The survey was developed based on a review of the available evidence base, identifying the key dimensions and indicators of ASRHR and selecting questions from existing, validated instruments and indicators typically required by funders or governments. The survey approached two strategies for addressing responses to sensitive questions. First, the survey was programmed on tablets and accompanied by an audio track digitally recorded into an ACASI program. Secondly, indirect questioning was used on best friend reporting on sensitive topics (e.g., whether their best friend engaged in the particular behaviour) and community prevalence (how many peers out of 10 they think engaged in this behaviour) were compared to self-report.
The COVID-19 pandemic prompted greater interest in the use of an ACASI approach as it reduces in-person contact and the technology used can be sanitized between respondents. Results based on data collected with the ACASI method was similar to that collected previously during face-to-face interviews in the SRH survey. Adolescent participants reported enjoying their use of the technology, potentially engaging more with the survey as a result, and having greater confidence in the confidentiality of their responses than during face-to-face interviews.
Vignettes
Vignettes were incorporated that explored gender attitudes, puberty, pregnancy and abortion attitudes and knowledge. The vignettes offer a wealth of information since questions can be looked at individually for gender non-conforming behaviour, for instance, but the existing scoring rubric also creates opportunities for easily characterizing responses at the level of gender attitudes and norms.
Adapted from the Global Early Adolescent study, the vignettes explored gender dynamics, gender in relationships and adolescent pregnancy and could be scored along a continuum to categorize responses. The results from the vignettes portray gender divisions along expected lines with girls expressing a more passive approach to relationships while boys were seen as the assertive protagonists, which has implications for gender-based and sexual violence messaging. Girls also had higher scores related to responsibility and acceptance of pregnancy than boys, underscoring that girls are disproportionately affected by the outcomes of pregnancy or abortion. There was also more discussion of the acceptability of abortion as an option in pregnancy than was found in other survey questions.
Household survey on maternal, perinatal and child mortality and service utilization
Due to COVID-19, funds were redirected to conduct a community-based survey. The face-to-face survey was conducted in Kisesa focusing on key indicators of reproductive, maternal, newborn, child, adolescent health and nutrition, with a modified instrument based on the DHS questionnaires. Being able to ask targeted questions about COVID-19 is a great example of a situation in which a local survey can be useful and necessary– to provide information on an emerging topic or an event of significance to SRHR but not included in national surveys. Overall, the partners’ experience highlights that it is possible to collect high-quality data with local surveys, though it is resource intensive.
Facility survey
The data collection strategy for the facility survey had two components. The first component was a questionnaire, adapted from the WHO’s Service Availability and Readiness Assessment (SARA) tool with an additional section on gender-based violence, adapted from an existing JHPIEGO instrument. Secondly, facility records were collected from September 1, 2018 to August 31, 2020. Although the facility survey is labour intensive and time consuming, it provides valuable information on the availability of services and drugs, as well as potential barriers to accessing services. In the review of registry data, adolescents (15-19) represented 38.9% of all cases of gender-based violence, 12.1% of all cases of STIs, and 16.9% of the recorded obstetric and gynecological cases, including antenatal care (12.7%) and delivery (12.1%). Inpatient records also show that complications of abortion contributed to adolescent hospital admissions.
Collecting qualitative data: Peer research
Specific ASRHR and gender transformative indicators, particularly at the immediate level, are best addressed by in-depth qualitative data. Therefore, partners designed and tested a peer research approach based on peer ethnography. This approach offers many advantages in terms of staffing as it needs fewer research assistants (RAs) than a survey and few technology needs, both of which reduce cost. It is also more flexible as peer researchers can have discussions with their friends at times and places not necessarily accessible to researchers. The approach allowed adolescents greater involvement in the data collection process while maintaining the focus on the research objectives. To facilitate rapid data collection, peer researchers worked one-on-one with trained, same-sex RAs over a specified period of time. The thematic analyses helped identify adolescents’ primary concerns pertaining to SRH, proposed strategies for engaging adolescents in health services and programs and identifying locations adolescents frequent and where they could be approached for participation in research or programs. The focus on “how” can also contribute to monitoring and process evaluation, by illuminating the ways in which adolescents interact with interventions. In the interviews with RAs, peer researchers mentioned feeling more confident discussing difficult topics with peers.
Key Partners
- Countdown to 2030, University of Manitoba
- Plan International Canada
- Africa Population & Health Research Centre
- National Institute for Medical Research
For resources and more information on this Lab, click here.
Lab 2: Harmonized Health Impact & Partnership Metrics to Accelerate Knowledge Sharing and Utilization

Challenge
Better creation, sharing and use of knowledge among all stakeholders are fundamental to addressing challenges affecting women, adolescents and children’s health (WACH). In order to reduce duplication, maximize functionality, and benefit civil society and academic collaborators, research partnerships must be carefully monitored and evaluated with an equity lens that considers the context of resource disparity. The use of tools developed for this purpose remains voluntary and there is no tracking mechanism in place to systematically collect and analyze data associated with the partnership process.
Key Issues:
- Knowledge exchange isolated and scattered: Effective and timely sharing of knowledge acquired by Canadian global health organizations with their global partners would reduce duplication of efforts and provide clearer research gaps for more efficient channeling of research funds.
- Data rich, exchange poor: A more comprehensive and integrated approach in traditionally siloed anglophone and francophone research communities is needed to foster collaboration and support real time informing of best WACH practices.
- Equity-level partnerships need data: Equity-centred partnerships hold greater potential for health impact and local development of capacity, yet outcome-level data for these partnerships from a Canadian WACH research investment are not available.
Results
Three bilingual tools were developed to address different needs.
Partnerships involve complex relationships between individuals and organizations, each with their particular positions, context, needs, resources, and agendas. In global health, partnerships are common between organizations in high-income countries (HICs) and those in low- and middle-income countries (LMICs). Such partnerships can be difficult to navigate, particularly because issues of power are rooted in complex sociopolitical and economic histories and a disparity in resources between HIC and LMICs. The proposed tool provides a mechanism for opening productive and relationship-building dialogue aimed at raising awareness and developing responses to the complex relationship and relational processes that lead to more equity-centred partnerships. The final EQT-GHP tool was completed along with an accompanying instruction manual and fact sheet.
Patient experience is recognized to be one of the three pillars of quality in healthcare alongside clinical effectiveness and patient safety. Broadly defined, patient experience encompasses effective communication, respect and dignity, and emotional support as experienced within a population’s health system. The purpose of this study was to provide a measurement tool that efficiently describes what a recently delivered mother has experienced as she can best recall. It is intended that the tool will assist health facilities in monitoring the experiential quality of care they are providing and to be able to compare findings among varied maternity care protocols and related services.
While the impact of male engagement in maternal and child health remains largely understudied, there is emerging evidence that educating husbands/partners about maternal and child health and facilitating their engagement does positively influence utilization of services, pregnancy and perinatal care outcomes, and a willingness to provide required financial support. This makes it all the more important to have access to a harmonized assessment tool that allows for baseline assessments, followed by the monitoring and evaluation of programs that aim to strengthen male engagement in health.
Key Partners
- Canadian Coalition for Global Health Research
- McGill University
- HealthBridge Foundation of Canada
- Université Laval & Regroupement stratégique en santé mondiale of the Réseau de recherche en santé des populations du Québec
For resources and more information on this Lab, click here.
Lab 3: Collecting Data on Sexual & Reproductive Health (SRH) in Humanitarian Settings

Challenge
Currently, the global forcibly displaced population exceeds 65 million people, with one in four being a woman or girl of reproductive age. Women and girls are at serious risk of death or disability due to SRH complications, including: unsafe abortion, a major contributor to maternal death and disability in humanitarian contexts; forced marriage; and, sexual violence. They are also at an elevated risk of acquiring HIV and other sexually transmitted infections. The lack of data on SRH in humanitarian settings is a critical global issue. This data problem presents challenges for effective resource allocation and timely service delivery, thereby impacting the health outcomes of extraordinarily vulnerable populations.
Key Issues:
- Data gaps: Consistent, reliable and rigorously collected data on SRH in humanitarian settings is sparse across the globe. This gap is even more pronounced when the SRH issue is politicized, such as with abortion data.
- Low data quality: The limited data that is available is often inconsistent, producing highly variable content and quality. Limited data and its poor availability also complicates the measurement of the impact of interventions, including life-saving interventions such as abortion, that take place during emergencies.
- Missing or inaccessible data: Currently, it is unclear what happens to SRH data that is collected in conflict settings, and whether the data is being used or can be used to benefit current or future humanitarian programming efforts.
Results
Multi-country assessments were completed in Afghanistan, Bangladesh, the Democratic Republic of the Congo (DRC), Jordan, and Somalia with a local organization/principal investigator in each country. The assessments indicated that the new global standards for abortion-related data collection are not being met, misconceptions about what is legally permissible with respect to data collection are rampant, and there is a lack of standardized tools/guidance for how to collect high quality facility-level data. Partners identified a number of priorities regarding other SRH indicators.
Partners continue to actively disseminate the findings from the Collaborative initiative. This has included: formal presentations at international conferences and annual meetings; global webinars; peer-reviewed journal publications; and five reports in collaboration with WHO. In addition, this Lab is working with Safe Abortion Care Sub-Working Group of IAWG and WHO on a special issue of Sexual and Reproductive Health Matters dedicated to abortion in humanitarian settings, and the findings from all five assessments. Led by National Abortion Federation Canada, partners will also submit a commentary on this Collaborative and the importance of bridging international engagement with federal stakeholders in Canada. This special issue will be published in late 2021/early 2022.
Since September 2019, lead Lab partners have worked closely with the Department of Reproductive Health Research of the WHO Geneva and the WHO country offices in Afghanistan, Bangladesh, the DRC, and Jordan, to undertake assessments on a comprehensive range of sexual, reproductive, maternal, newborn, child, and adolescent health indicators. The aim of this larger project is to develop a core set of indicators for routine collection in humanitarian settings. The tools and materials dedicated to facilitating abortion-related data collection will be incorporated into these broader efforts. In addition, the WHO group will convene meetings for stakeholders in both South Asia and West Africa, and country-level meetings in Afghanistan, Iraq, and Jordan to present the findings and discuss next steps.
Engagement with IAWG and the Safe Abortion Care and Research and Data Sub-Working Groups (SAC-SWG)
As a key partner in this project, the Inter-Agency Working Group on Reproductive Health (IAWG) supported the active engagement of member agencies. In November 2019, a meeting of the SAC-SWG was convened to provide information about the expanded project and to discuss the preliminary findings from the early assessments. Partners strategized about the SAC-SWG side event at the 2020 IAWG meeting and a delegation from Jordan as well as partners from Bangladesh were to be supported to advance abortion-related data collection and advocacy in both sites. In addition, partners spent fall 2019 organizing a Research and Data Sub-Working Group event for the IAWG meeting. Through this session, partners engaged with global stakeholders about both the abortion-related findings and the larger project with WHO. Finally, partners had planned to organize a workshop in Bangkok in conjunction with the 2020 IAWG meeting to finalize the tools for abortion-related data collection.
Due to the COVID-19 situation IAWG postponed the annual meeting. As a result, partners have pivoted and are now working with SAC-SWG delegations from Bangladesh, the DRC, Jordan, and Pakistan. This ongoing engagement includes providing support to stakeholders to integrate data collection on abortion into routine surveillance.
Key Partners
- University of Ottawa
- National Abortion Federation Canada
- Inter-Agency Working Group on Reproductive Health in Crises (IAWG)
- World Health Organization, Department of Reproductive Health Research
For resources and more information on this Lab, click here.
Lab 4: Maximizing use of existing data to strengthen program design, evaluation & impact
Challenge
National and international non-government and civil society organizations spend substantial time and resources collecting data in order to design and monitor their health interventions. However, estimates of numerous health and social indicators in many countries already exist in publicly available datasets, such as the Demographic and Health Surveys (DHS) and the Multiple Indicator Cluster Surveys (MICS). DHS and MICS provide standardized data collected using rigorous methods, well-trained enumerators, and large sample sizes. Among the challenges of using publicly available data to assess baseline conditions is that they are rarely designed to be representative of district and village contexts, where non-governmental organizations (NGOs) are often working. In addition, DHS and MICS are collected every three to ten years so there may be a gap between when data was collected and current baseline conditions.
Key Issues:
- Responsive to context: Adequate assessment of baseline conditions is especially important to ensure interventions respond to the varying health needs within populations and promote equitable policies.
- Increased data use: Utilizing publicly available data to meet baseline data needs can, in turn, increase the use and quality of publicly available data (collected regularly) to better inform program design, implementation, evaluation and learning.
- Data-informed decision-making: Maximizing the use of available data strengthens the capacity of researchers, NGOs and in-country leaders to collect, analyze, and inform programmatic decisions.
Results
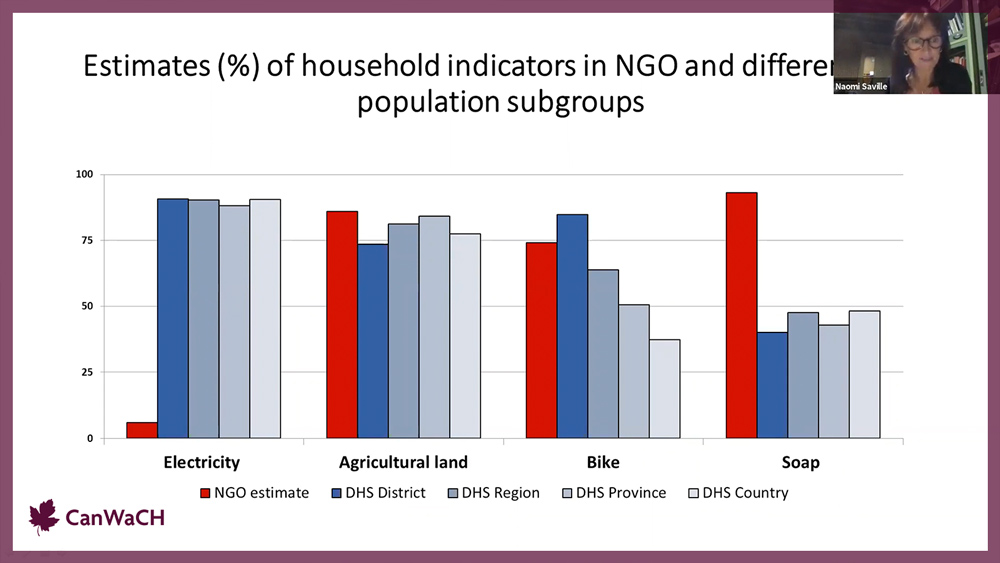
Analysis of NGO vs DHS/MICS
The objective of these analyses was to compare the indicator estimates from NGO baseline reports to indicator estimates calculated using publicly available data (DHS or MICS). A sample of 46 NGO baseline reports from MNCH projects carried out in 23 low- or middle-income countries were compiled. From the reports, partners extracted: country name, NGO name, date of beginning and end of data collection, population of study and inclusion and exclusion criteria, indicator name, sample size (total and used for each indicator), location of data collection, and the indicator estimate. DHS (from twenty countries) and MICS (for surveys from three countries: Vietnam, Laos, and South Sudan) indicator estimates were matched with the estimates from the NGO surveys, matching geographic level as closely as possible. In total there were 139 indicators, grouped into 41 subgroups, matched between NGO reports and DHS/MICS.
Analysis of DHS vs DHS
Partners compared DHS data across multiple years or multiple regions, to examine the sources of variation in differences in the estimates due to sampling error, year of data collection or geographical level, but not in methods (because the DHS methods are largely consistent across surveys). DHS data from seven countries were used: Bangladesh, Ethiopia, Kenya, Malawi, Pakistan, Tanzania, and Zambia, and the same indicators as were used in the DHS/MICS vs NGO analysis were retained. DHS indicators from different cycles and geographical levels were matched using different combinations mimicking the actual DHS/MICS-NGO scenarios: indicators from the same level but different years (Scenario 1), indicators from the same year but different levels (Scenario 2), and indicators from different years and levels (Scenario 3).
Conclusion
The first hypothesis was that publicly available data can provide estimates of baseline conditions similar to those reported in NGO baseline reports when matched as closely as possible for location, year, and season of data collection. Partners’ answer to this is that publicly available data can be used if the NGO is tolerant of imprecise estimates.
While an NGO may use the evidence presented here to justify forgoing their own baseline survey, they should keep in mind that DHS and MICS provide estimates for only some of the indicators of interest to the NGO. On average, partners estimated 18 of the NGO’s indicators using DHS/MICS, but NGOs were often reporting 100+ estimates, which may justify their carrying out a full baseline survey. Furthermore, being in the field can provide valuable insights for project design and implementation. While partners cannot give a blanket recommendation that DHS and MICS could always replace NGO baseline surveys, there are some situations where DHS/MICS could be used to the NGO’s advantage:
- When the estimate is expected to be less than 15% or above 85%;
- When the indicator of interest is one of the few with consistent similarity between DHS/MICS and NGO estimates;
- When the NGO has tolerance for estimates of low or unknown accuracy and does not need estimates for all 100+ indicators.
The second hypothesis was that the impact of differences in year, geographical level, and season varies across health indicators. Project partners’ answer to this is yes (except for season), but the variation due to year, geographic level and health indicator is only a small part of the total variation, and even after accounting for those sources of variation there will still be differences between the estimates from the two data sources.
Key Partners
- HealthBridge Foundation of Canada
- Université de Montréal
- Centre for Creative Initiatives in Health and Population
- International Nepal Fellowship
For resources and more information on this Lab, click here.
Lab 5: Improving gender equality and nutrition data for women, children and adolescent girls

Challenge
Good nutrition and gender equality are mutually reinforcing: improving nutrition is critical to achieving gender equality, and vice versa. Empowerment of women and girls is identified as an important nutrition-sensitive strategy to address malnutrition in low- and middle-income countries. However, there is no established measurement framework to assess how nutrition and empowerment interacts and affects diverse communities and across nutrition interventions. These data problems prevent us from fully understanding the influence that empowerment has on women and adolescent girl’s nutritional status.
Key Issues:
- Research gaps: There are gaps in the relevant literature on empowerment and its effects on girls’ nutrition. Currently, no existing studies have focused on or even included unmarried and/or adolescent women.
- Lack of data and tools: Indicators of gender equality may only be collected in national surveys, such as Demographic and Health Surveys (DHS), which occur infrequently and may only collect data on women 15-49 years. This lack of consistent data does not support individual program interventions and course corrections.
- Lacking indicators: Lacking indicators on the interaction between nutrition programs and gender equality, and methods to frequently measure these indicators for program design, prevents programming from being responsive.
Results
The project undertook research into gender equality and women’s empowerment (GEWE) links to nutrition status and potential indicators that could be measured to identify whether the most GEWE-vulnerable beneficiaries are being reached through gender-sensitive nutrition programs, and eventually whether gender-transformative nutrition programs are having a positive impact on beneficiary’s GEWE status.
The project also led updates to the Nutritional Intervention Monitoring System (NIMS) toolkit. This included research identifying best-fit-for-purpose rapid assessment tools and survey designs monitoring needs. This is specific toward assessing the most appropriate program specific surveillance tools with monitoring indicators and context-specific indicators that could be collected across each project lifecycle.
Positive feedback from survey teams and country-level project officers indicated that the outputs from this collaboration strengthened the harmonized NIMS toolkit, reduced the workload during tool development and mapping of indicators to questions, made data quality metrics clear and transparent, and filled a critical need for evidence-based gender equity and women’s empowerment (GEWE) indicators in program surveys – beyond the classic ‘sex disaggregation’ of data.
The overall project and activities have allowed partners to reduce the resources or cost required to implement each NIMS survey (tools pre-set, methods transferable across countries); the use of harmonized tools, templates and checklists has increased the quality or “rigour” of survey outputs; the harmonized tools are easy to adapt, and to identify where adaptations are required for each country. All of these have made it more feasible to conduct surveys more frequently, but in particular, these same tools are being adapted for use more frequently in a routine monitoring format. Activities include:
- Development of an explanatory statistical model incorporating potential links between gender inequality, increased nutritional needs, and inequitable access to nutrition and health services, particularly among adolescent girls.
- Conducted two systematic reviews to help create a framework for measuring and linking gender and nutrition related outcomes.
- Identified simple appropriate indicators of gender equality to test in country settings.
- Program specific surveillance tools created: a harmonized checklist of recommendations and procedures to implement survey data, and a database for tracking survey data across time in an easy-to-use and transparent format.
- Included gender-related questions and indicators in the updated NIMS survey tools during the 2019-2020 round of country surveys, and was able to implement the updated NIMS in seven countries.
The project engaged fellows and early career researchers in the research and tool development activities. This helped to build sustainability in expertise in GEWE and nutrition research beyond the scope of the project by providing practical skills and application-oriented project opportunities. Due to COVID-19, in-person workshops were not conducted. Instead, the focus was to train staff who work directly with local government staff and survey partners to ensure that staff are sufficiently trained to disseminate findings and explain the procedures applied to data collection and analyses.
Key Partners
- University of Toronto
- Nutrition International
- Campbell Collaboration
For resources and more information on this Lab, click here.
Lab 6: Improving the Measurement of Sexual and Reproductive Health and Rights, Women’s Empowerment and Gender Equality in Humanitarian Settings
Challenge
Health program delivery and its measurement in conflict-affected and humanitarian settings is difficult to assess to ensure accountability. There is a minimum set of process measures but they are of unverified quality, especially depending on the type of conflict. Access for data collection to most affected populations is complicated due to ongoing security issues, which often disrupt routine data collection. Logistical and monetary costs of traditional data collection methodologies can significantly increase due to the added security costs, communications challenges and increased costs of human resources in humanitarian and conflict-affected settings. To streamline data collection and measurement processes, simpler approaches to valid and reliable gender-relevant analyses need to be identified.
Key Issues:
- Data Uptake: Identifying data practices, best data sources, and tools for planning will avoid duplication, reduce waste, and increase uptake of the information at early stages of developmental assistance, including investment planning stages.
- Strengthen Data Capacity: Standardize and simplify stakeholders’ capacity, including the next generation, in order to: select indicators; collect data; analyze data; communicate situation analysis and progress using strategic indicators; and, use data and indicators effectively.
- Expanding Health: Gender-relevant outcomes are influenced by a complex web of actors and issues that stretch beyond the health sector. Exploring indicators from multiple sources of data that are not traditionally assessed by the health sector can facilitate complementary gender equality change affecting the social determinants of health (e.g. education).
Results
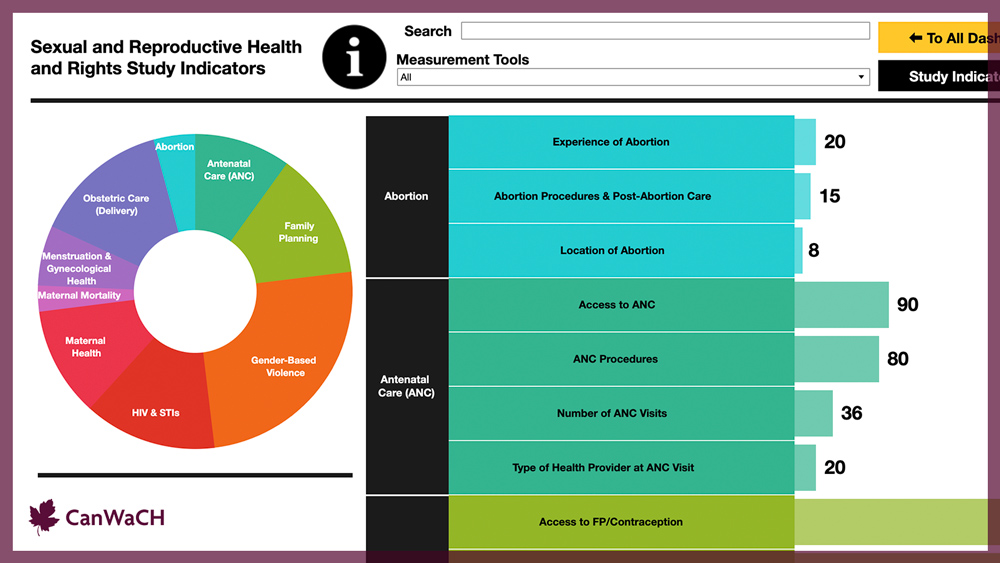
The project documented existing approaches to the measurement of SRHR and GEWE indicators in humanitarian settings, by conducting two scoping reviews. The first scoping review search, on the measurement of SRHR in humanitarian settings, yielded 385 publications and reports. SRHR indicators were categorized into nine domains: abortion, antenatal care, family planning, gender-based violence, HIV and sexually transmitted infections, maternal health, maternal mortality, menstrual and gynecological health, and obstetric care (delivery). A total of 65 tools and questionnaires measuring SRHR were identified, of which 25 were designed specifically for humanitarian settings. Although gender-based violence and pregnancy continuum indicators were well measured across humanitarian settings, several gaps in measurement were identified.The second scoping review search, about the measurement of GEWE in humanitarian settings, retrieved 170 publications and reports. Extracted indicators were categorized into seven domains: economic, health, human development, leadership, psychological, security and justice, and social/cultural. Thirty-eight toolkits and questionnaires were identified in this review, of which 19 were designed specifically for humanitarian settings. Social/cultural was the largest domain represented in this review, with gender-based violence indicators reported in 66% of studies. There was little representation of economic, human development and leadership indicators.
Two pilot studies were conducted. The first pilot study involved developing a machine learning software for title and abstract screening to be implemented during a systematic or scoping review process. While conducting the two literature reviews for this project, a need was identified to facilitate and improve the abstract screening process. For the literature reviews, a combination of existing machine learning approaches and developing new machine learning approaches were used. Literature reviews were completed from a wide range of collaborators and evaluated the performance of different textual embeddings and algorithms on predicting the inclusion of an abstract. The hope is for machine learning to become a routine aspect of systematic and scoping review screening, to increase efficiency and to minimize project workloads.For the second pilot, a logistics simplification and data reduction of SRHR indicators were conducted in Demographic and Health Surveys (DHS). The aims of these analyses were to evaluate if using a reduced sampling fraction of households and enumeration areas could generate valid estimates, and to monitor the progress of low- and middle-income countries regarding sexual and reproductive health, using a simplified version of selected Countdown 2030 indicators. This pilot found that it was possible to reduce sample size (both enumeration areas and households) when measuring some SRHR indicators, and that it is possible to reduce the number of questions asked when measuring more complex SRHR indicators. Using simplified versions of the health indicators could reduce the amount of information needed to be collected, reducing survey length and the overall time to conduct a DHS survey.
Interactive dashboards were created to showcase the tools, indicators and gaps found in both reviews. The dashboards were created using Tableau, a software which allows for the creation of open platform, interactive dashboards in a story format. The dashboards are a synthesis of data collected on measurement tools, methods, and indicators extracted from the scoping reviews, with both coverage and outcome indicators included. As a whole, these dashboards provide an inventory of available toolkits and indicators relevant to SRHR and GEWE and their data sources, which can be sorted by topic, country, humanitarian setting, study design, or study method.
Key Partners
- SickKids Centre for Global Child Health
- Canadian Red Cross
Looking Back, Looking Forward
As part of CanWaCH’s development of our strategic plan, we consulted numerous stakeholders including member experts and external thought leaders in monitoring, evaluation, research, and learning. Our aim was to better understand and identify emerging priorities for capacity strengthening and knowledge sharing, and resulted in several exciting outputs in 2021, including but not limited to:
- Technical Guidance Note on Measuring Women’s Empowerment in the Global Health Sector: a practical resource and accompanying video tutorial created for all global health initiatives seeking to measure empowerment in their work.
- Critical Dialogues Series: leveraging the findings of the Collaborative to further explore adaptive shifts in data methodologies, guidance and lessons learned.
- CanWaCH at the IATI VCE: CanWaCH’s contributions to the International Aid Transparency Initiative (IATI)’s Virtual Community Exchange (VCE) events this year focused on mapping, visualizing and analyzing data more effectively (VCE1), as well as on the importance of accessible data in gender financing (VCE 2).
- The Network Map: Building on the successful Project Explorer platform, the Network Map was developed to track Canadian organizations, groups and projects working to advance gender equality domestically.
Beyond these outputs, CanWaCH identified several areas where additional exploration would be useful for the sector. These will be reflected in our work and analyses in the months ahead:
- Integration of decolonization and local leadership in monitoring, evaluation, accountability, and learning mechanisms. Building on learnings from the 2021 Global Health Impact Report, it is evident that increased integration of anti-colonial, locally-led approaches is a priority for Canadian development organizations and their partners. Focusing specifically on the role of monitoring, evaluation, and data, some areas for future investigation and analysis include:
- Strengthening integration with, and investments in, global and local health information systems within the countries in which Canada partners.
- Improved access to information by, and about, the diversity of partners with whom we work, and an increased recognition of their leadership.
- Specific and targeted skill building and knowledge sharing of anti-racist, anti-colonial, and feminist methodologies and orientations, as well as a critical reflection of what is needed to be able to action these within our own organizations.
- Supporting technical capacity with regard to developing monitoring and evaluation plans and strategies. Early in 2022, CanWaCH will be producing technical guidance for the sector to support the development and ongoing refinement of monitoring and evaluation plans, particularly for those projects funded by Global Affairs Canada. In developing this guidance, we have uncovered a few specific areas where additional support may be useful.
- Increased practical guidance regarding the development of effective and comprehensive learning and dissemination plans in global health programming.
- Consistent understanding of, and engagement with, ethics review and approvals in Canada and globally, across partners and projects.
- Increased availability of best practice resources for integration of various methodologies (particularly virtual practice, qualitative methods, and mixed methods approaches) in global health programming.
In addition, specific areas of topical interest include: integration of climate, environment, and global health; rights-based issues in connection with global health; neglected areas of sexual and reproductive health and rights; data management and collection in humanitarian settings and fragile contexts; and data sharing and transparency for accountability. More broadly, consideration of how COVID-19 has influenced (and continues to influence) how we work, research, and evaluate remains at the forefront of people’s minds – not just in terms of processes, but also in terms of human resources and capacity needs as the sector evolves. In the coming year, CanWaCH will reflect these and other emerging priorities in our data work, specifically through the generation of technical guidance, increased sector data collection, and critical analyses.
Acknowledgements
This report was developed by the Canadian Partnership for Women and Children’s Health (CanWaCH). In particular, we gratefully acknowledge the contributions of Jessica Ferne and Imaeyen Okon. Thank you to Tina LaRochelle, Klaudia Rymaszewski, Mélody Tondeur, Erin Jex, and Julie Vautour for their support with literature review, data entry, analyses, and outreach. We also appreciate individuals from the various organizations and institutions who took the time to provide insights and resources that informed this report, as well as all those who contributed data to the Project Explorer during the past year.
Comments or questions on this report may be directed to [email protected].
Disclaimer
The insights and data referenced in this report have been provided by contributing organizations, and have not been independently verified by CanWaCH. Numbers are accurate at the time of publication, and may change as projects are updated. As such, the figures in this report may differ from current data shown on the website. CanWaCH does not endorse or recommend specific programs or activities, and the content of this report is intended to be inspirational and not prescriptive.
The designations and maps in this report or on our website do not imply the expression of any opinion whatsoever on the part of CanWaCH concerning the legal status of any country, territory, city or area or its authorities, or concerning the delimitation of its frontiers or boundaries.